
The Dilemma of Nerve Pain
-

I specialized in biomechanics and designing functional foot orthoses. Patients would present with a great myriad of lower extremity symptoms and I had to determine if I could help them. I learned a lot from getting them into more stable shoes, low dye taping, varus or valgus wedges, and OTC arch supports that I could modify at will. Yet, these measures address mechanical issues of over-pronation, over-supination, limb length discrepancy, poor shock absorption, and weak muscles, but seem to be at odds when the source of pain in nerve pain.
To review, we pretty much need to get good as clinicians in diagnosing and treating mechanically induced pain, inflammatory induced pain, and neuropathic causes of pain. At least, we need to make the appropriate referral. But these are the big 3, yet they are still only 3 (and not 12 so we should be able to handle).
Let's take a patient with Morton's neuroma, that actually has an ultrasound or MRI documentation of a Morton's neuroma. This a classic nerve problem, with neuropathic pain being generated, that we have to treat. What is Occam's Razor (Simpliest Solution) for Morton's Neuroma in the Podiatry world out there? I assume it is a good orthotic device with a Metatarsal Pad to spread the metatarsals apart. This is typically your Plan A which is the role of Occam's Razor in the First Place. Create Plan A. Here we have a Nerve Problem with a primary Mechanical treatment. Which works half of the time, maybe more. What is the typical Plan B? Cortisone shots, icing, contrast bathing, NSAIDS, etc. These can double your odds for success so now we have helped 75% of all Morton's Neuroma patients that walk through the door. This is always fascinated me! I am easily entertained! Here we have a Nerve Problem with Plan A and Plan B, at least how I learned it, being Mechanical and Inflammatory treatment categories.
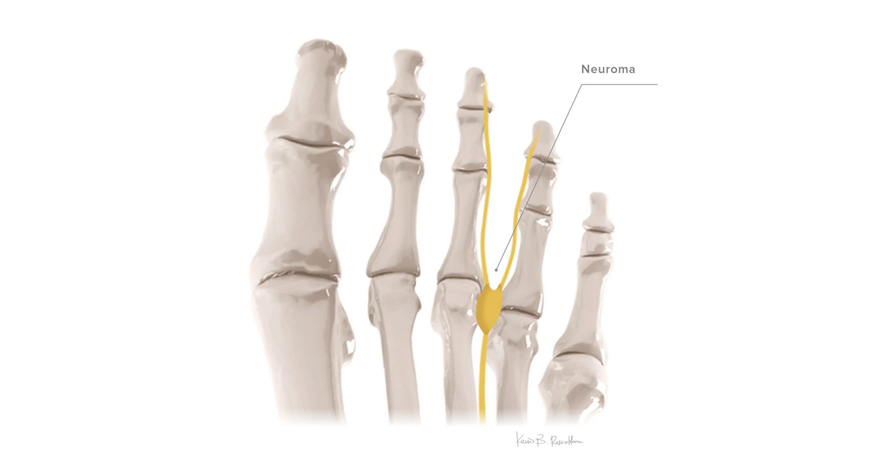
So, here is the fascinating part. We have helped significantly 75% of the patients, and the patients that do not respond typically get surgical intervention to remove the Neuroma. Wait a minute please! There is that 3rd source of pain called Neuropathic Pain. We know that neuropathic pain is many times treated very well by mechanical and inflammatory treatments, but the remaining 25% should have a trial of nerve treatments. You could easily say that I have been doing it backwards even my whole life (since this was my approach to Neuroma pain for decades). If a patient presents with nerve pain, even in the documented MRI neuromas, perhaps we should start with nerve treatments.
Every since Dock (Dr Gary Dockery) introduced alcohol injections into Podiatry, I have had fun with de-sensitizing nerves with various concentrations of alcohol. Tens units should be a part of this de-sensitizing, and well as neural flossing, topical OTC nerve lotions like Neuro One (designed by Dr Arlene Hoffman), Rx Compounding concoctions, and even evening dosing of Lyrica or Gabapentin (to start). Now, the patients requiring surgical removal are in single digits. There is an association of Neuropathic Physical Therapists to send your patients to also.
And, remember that nerves in the foot are connected by a superhighway to the low back, cervical spine, and brain. So, there are many instances that the nerve pain in the foot is referred pain from the spine (somewhere). I have countless foot nerve pain patients that could not wear their great custom orthotic devices designed by me due to heel or arch hypersensitivities only to get better with lumbar, thoracic or cervical disc treatments.
So, whether you are thinking nerve pain or not initially , when the patient response to your custom orthotic devices is displeasure from too much pressure in some area, when the majority of your other patients tolerate that support just fine, think nerve hyper-sensitivity, and then nerve treatments.
In conclusion, nerve pain can be treated with mechanical changes and anti-inflammatory approaches, but may need a combination of these with select neuropathic treatments. Nerve pain may also not respond, or get worse with mechanical change attemps, and will need straight neuropathic treatment until the nerve involved is calmed down. An heightened index of suspicion is needed when treating the foot with mechanical changes if the patient responds negatively to something that seems other patients would have no issue with. Common issues of Morton's neuroma, metatarsalgia with nerve symptoms, arch pain, heel pain, tarsal tunnel or medial ankle pain, are common areas that can respond mechanically and with inflammatory measures, but may need neuropathic treatments and workups.
The last comment on nerve pain today. Any chronic problem, say sesamoid fracture slow at healing for example, is a mechanical and inflammatory issue, but after 3 months if the pain level has remained too high, neuropathic hyper-sensitivity can set in and need to be addressed.