
Using the Configurator in FootID Pro, Part 7
-

The most recent entry in this series of discussions focused on the rearfoot posting options within the FootID Pro application. The next field we will discuss is “Forefoot Post”. As I stated earlier, it is my belief that posting an orthotic device properly is a main differentiation between a fully customized and prescribed foot orthotic device and a less effective off the shelf foot support. A foot orthotic device should function throughout the stance phase of the gait cycle, heel contact, midstance through propulsion and toe off. Creating a stable base in the forefoot from which the lower extremity can forcefully contribute to the ability of the entire body to move forward should be a primary goal of foot orthotic therapy. A trained practitioner should be able to evaluate any forefoot condition, whether it be forefoot varus, supinatus, valgus, plantarflexed 1st ray, hypermobile 1st ray, as well as variances in the metatarsal parabola. This leads us to the question of how we address these various conditions, and the answer generally lies with the use of forefoot posting.
The field “Forefoot Post” within the FootID Pro app is similar to the rearfoot post field. There is a toggle to choose either extrinsic or intrinsic, as well as either valgus or varus. There are options for zero, two four and six degrees, although generally you can post up to 8 degrees of forefoot deformity. For most models there is a default value in this field, so look for the orange checkmark. The chainlink icon, if selected to allow you to differentiate left and right versus a bilateral value.
Intrinsic forefoot posting is far more commonly used than extrinsic posting. Long gone are the days when I was a young podiatrist, when we used Rohadur plexiglass for our orthotic frame with acrylic extrinsic posts in both the rearfoot and forefoot. These devices were bare bones, and hard to get used to, especially if you have a mild gastroc equinus and forefoot supinatus like I do, but they worked! It is my belief, as well as others, that we should strive to encourage motion primarily directed on the sagittal plane during propulsion as much as possible, and limit less effective, and sometimes pathological frontal (rolling in and out) and transverse (twisting in and out) plane motion. It is profoundly important to understand the underlying mechanical causes of common forefoot maladies such as Hallux Abducto Valgus, lesser metatarsal issues, Morton’s neuroma, hammertoe and tailor bunion deformities, all of which can be alleviated with orthotic devices with built in forefoot correction, often coupled with other treatment protocols.
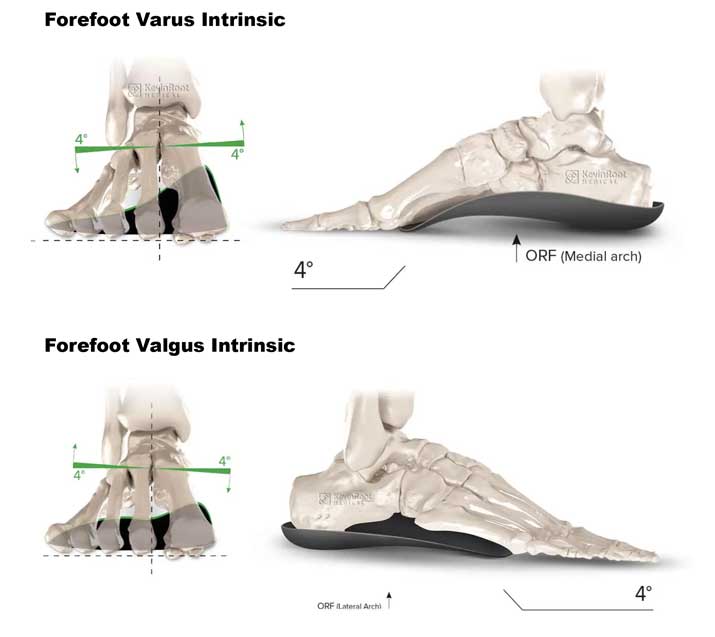

These four web pages are also available on the KevinRoot Medical website in one page PDF form for easy reference material. A description of balancing the forefoot to rearfoot is on the varus intrinsic post page, I highly recommend reviewing this for those of you not familiar with this concept.
It should be noted that intrinsic forefoot correction is performed either physically to the positive mold before pressing the frame, or digitally in the positive scan of the foot. The extrinsic post, (extrinsic bar) is added to the frame after pressing, and is usually made of rigid or semi rigid EVA similar to rearfoot posts. Extrinsic posts, especially higher than 2 degrees of correction can create a ledge or drop off in the distal edge of the frame in the location of the thickest portion of post. I have found it beneficial to combine extrinsic and intrinsic forefoot posting in high degree deformities, particularly in varus or supinatus conditions, generally using a 4 degree extrinsic bar and balancing the rest of the deformity intrinsically.
Another clinical pearl is the use of the tip post, which is a small triangular post placed under either the 1st or fifth metatarsal. Tip posts help prevent the front edge of the orthotic frame from sinking or cutting into the sock liner or midsole of the shoe, particularly in athletic shoes, thus losing correction and causing damage to the shoe. They also create stability to the distal edge of the frame when using 1st or 5th ray cutouts.
The effective use of posts, as alluded to previously, is a main difference maker between a true custom foot orthotic and an off the shelf generic foot support. Another difference maker is the expertise of the biomechanics practitioner., The ability to perform a thorough evaluation prior to the manufacture of the orthotic devices, an accurate and effective prescription addressing the particular patients biomechanical issues and symptomatology, as well follow up and evaluation of the ultimate performance of the orthotic devices. Adjustments to orthotics are commonly necessary, based on clinical judgement, and should not be viewed as a failure or deficiency. Adjusting posts is often an easy and effective way to enhance the performance of your custom foot orthotic devices.