
The Metatarsal Arch Deformation and Forefoot Movement in Gait: A Study of the Kinematics (Motion)
-

This study is excellent in describing the forefoot motion during contact/midstance and then propulsion. The authors are able to separate the forefoot into 3 segments: 1st metatarsal alone as the medial segment, 2nd and 3rd metatarsal as a central segment, and 4th and 5th metatarsals as the lateral segment.
Here is what we already know a lot about!
The longitudinal medial arch flattens during early stance with the metatarsals dorsiflexing due to ground reactive forces, and raises in the later part of stance with the metatarsals plantarflexing. This we know and validated by this study. This is the sagittal plane motion of the foot.
Yet, what then happens in the transverse and frontal planes during the later part of stance?
Let’s first look at this diagram from the article.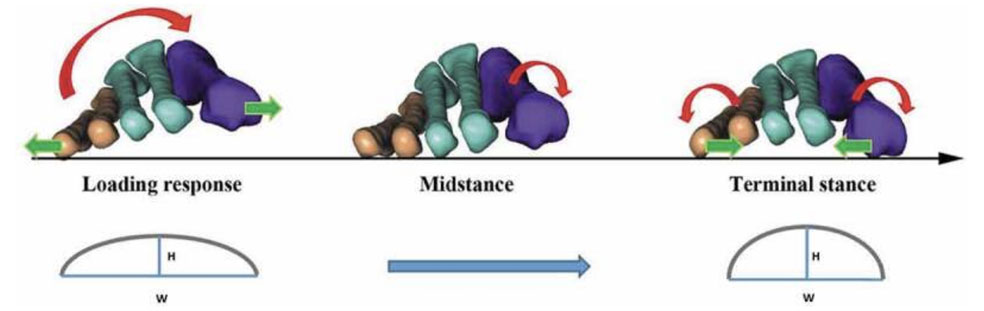
Here we see the contact phase with the foot’s loading response first. The metatarsal arch will lower in height and the metatarsal width widens. This structure stays fairly stable in mid stance with propulsion (here termed terminal stance) seeing a rise in the metatarsal arch due to abduction of the first metatarsal and adduction of the fifth metatarsal. This is coupled with the inversion of the fifth ray and eversion of the first ray.
I will summarize their data.
Medial Forefoot (1st metatarsal)
Initially DF, Ev, Adduction (peak DF 70% of stance)
Then PF, Ev, Abduction (peak eversion 85%)
**Dr. Blake’s comment: This is possible since the main activity of eversion is at the talus and navicular, so the inversion occurring in the first ray is still seen as overall eversion to the ground.
Central Forefoot (2nd and 3rd metatarsals)
Initially DF, Ev, Add (peak DF 72% of stance)
Then PF, Inv, Add
Lateral Forefoot (4th and 5th metatarsals)
Initially DF, Ev, Abduction (peak DF 71% of stance)
Then PF, Inv, Adduction

Here are all the sensors that they put on the 30 subjects to record their data.
The Medial Longitudinal Arch Angle went from 126 to 146 by 70% of stance (flattening of the arch) to rebound to 131 at Toe Off (re-supination)
The Metatarsal Arch Height standing on 2 feet (Bipodal) was 14 mm with range 8-22. The highest arch was at 87% with changes of 0.87 and 1.32 mm while walking.
The Metatarsal Arch Width had a mean of 104 mm with a range of 92 to 130 mm. The width changed around 1 mm from 21% to 71% of stance.
In general, both the medial and lateral sides of the forefoot everted in contract phase relative to the ground. During the contact phase, the first metatarsal adducted towards the midline, thus had to be inverting around the first ray axis. The fifth metatarsal in contact abducted away from the midline around its axis. The peak drop in the navicular was somewhere between 73 to 77% of stance. This is later than the metatarsal signs that pronation had stopped therefore hinting that foot resupination starts at the forefoot, not the rearfoot. Another interesting point is that the plantarflexion of the metatarsals in resupination occurs more in the medial and central metatarsals over the lateral metatarsals. It seems to me that the resupination process is anchored in a stable cuboid and the 4th and 5th metatarsals which barely move from forefoot loading to heel lift.
One final point to bring up is the role of the muscles in this process. The intrinsics will be working hard to stabilize the metatarsal area. The stronger your intrinsic muscles the better for that process. Then the posterior tibial and peroneus longus need to stabilize the midfoot, holding the metatarsal plantar grade so that heel lift can occur. Now, a strong achilles complex can pull up the heel and allow the MPJs to have a solid pushoff.