
Cuboid Syndrome, Observations and Comments
-

Last week’s blog post presented a case study of Cuboid Subluxation secondary to plantar fascia rupture. Commonly present as associated with or secondary to other conditions, such as plantar fasciitis or lateral ankle instability, it can also be present as a standalone (pun intended) condition. My career in podiatric medicine spanned from 1980 to the early 2020’s, during which I noticed a remarkable uptick of Cuboid subluxation occurrence during the latter years of my career, as well as relatively more cases of plantar fasciitis and 2nd MTPJ capsulitis. Why is that? During the initial years of my career I wore dress shirts, neck ties, a long white lab coat, and leather dress shoes to work in my office everyday. Fortunately, over the years, I was able to do away with the neck tie first, then the lab coat, and eventually the dress clothing to much more comfortable scrubs made from light weight athletic clothing type material and my favorite running shoes (Brooks Adrenaline). During that time span, many people also switched to lightweight athletic type shoes for everyday wear, shoes with very little structure to them, offering a very cushioned feel, but mainly reliant on the EVA midsole without a stiffer outer sole to maintain whatever stability the shoe possessed. Additionally, many models of shoes featured a “foot bridge” or narrowing of the midsole at the midfoot, in between the heel and ball of the foot causing additional decrease in the longitudinal and torsional stability of the shoe. Why did this happen? My hypothesis is that shoe manufacturers need to constantly come up with new features to remain competitive, but they also found this construction technique saved costs for materials and simplified the manufacturing process for athletic type shoes. The result was cheaper shoes, but more incidences of Cuboid subluxation.

Since my generation of baby boomers favorite shoes of heavy, white leather upper New Balance cross trainers (with white crew socks) is slowly disappearing into the dust bin of history, more and more people are wearing lightweight shoes with EVA missiles, even now with men’s business attire. So, how do you avoid provoking a Cuboid subluxation situation? Normally, the foot acts as a double hinge on the sagittal plane during the stance phase of gait.
The first hinge is the ankle joint as the lower leg rotates forward over the foot which is fixed against the ground after heel contact.
Then as we progress into propulsion the second hinge is at the level of the metatarsal phalangeal joints as the rear foot lifts off of the ground and rotates forward over the ball of the foot and eventually the toes.

However, in certain cases, such as hypermobile feet with tight posterior muscles, an intermediary bending force can occur at the level of the midfoot, and unless this bending force is resisted, Cuboid subluxation can occur, where the Cuboid follows the downward bending of the rear foot, and the 4th and 5th metatarsals are bending upward by the ground reactive force under the fore foot. Concurrently, the Peroneus Longus is activated during this time, and as it coursed laterally to, and then beneath the Cuboid, it can apply an eversion force to the Cuboid if the foot is unstable.
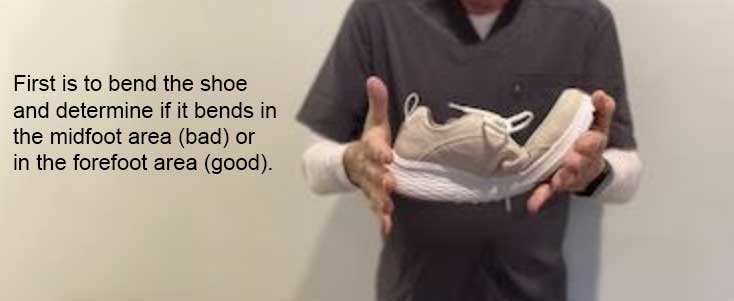
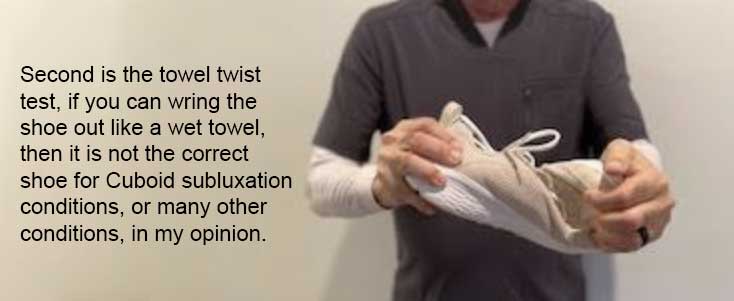
There are two simple tests to check if a shoe is stable enough to resist these forces and assist in preventing Cuboid subluxation.
However, a side benefit to using a full length, functional orthotic within the shoe is to provide some added stability within the shoe, resisting the midfoot weakness longitudinally and torsionally inherent to the shoe.

A well placed Cuboid pad placed under the Cuboid bone, either as part of an orthotic or within a low dye strapping of the foot provides remarkable stability to the Cuboid. This is demonstrated by placing a finger under the Cuboid with the patient standing, and noting how elevating the Cuboid stabilizes the 4th and 5th rays against reactive ground force under the metatarsal heads.
In summary, we place an emphasis in foot biomechanics on creating stability within the medial arch of the foot, but a “lateral arch” also exists and should not be disregarded.
-
-