
P2 Pathology Based Orthoses: Adult Acquired Flatfoot Design
-

Patients with this foot type who present to you may bring a whole bag of unused orthotic devices with them. They have pain in their feet somewhere which brings them to see you, but further questioning can elicit pain in many other areas of the lower extremity up to the low back. The shape of their feet does not like to be forced into a given shape, therefore generally their shape must be supported to prevent further joint breakdowns (Orthotic Goal #1). You are supporting, preventing joint subluxations, but not changing shape with the P2 design.
What are the great components of the P2 design? These are:
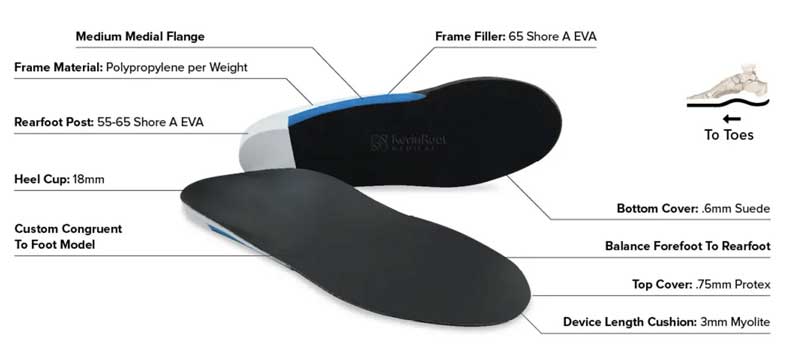
- Solid Frame with Polypropylene
- Deep Heel Cup
- Solid Rearfoot EVA Post (typically with no motion)
- Molded to the Patients Foot with FF to RF balancing
- Frame Fill Rigid (can be reduced or removed if pain in the arch)
- Top Cover and added Full Length Cushioning with Myolite
What are the most common modifications that are added to the RX of a P2? These include:
- With heel valgus, you can attempt some varus re-alignment with 4 mm of medial heel skive and changing the heel cup height to 21 mm with a low and standard length lateral flange
- Also with heel valgus, this re-alignment can be done with the Inverted Technique. Most start with 25 degrees of inversion, 21 mm heel cups, and medium lateral flange to met shafts
- When these patients present with arch prominences (like sub navicular or first cuneiform, you can ask that the frame has a punch out, like for the navicular shown here When you use buttons to reduce pressure plantarly I would rather not use any frame fill for ease of in-office adjusting. I would rather use 3/16 inch or 4.7 mm polypropylene to achieve the desired rigidity.
- Also, since these feet tend to bulge medially in the arch and splay laterally in the forefoot, containing these feet with wide arch profile frames and long and high lateral flanges can make a big difference in their mechanics
Hope this discussion can help you in your decision making of Adult Acquired Flatfeet.
Rich